Specialty Focus
Peripheral Nerve Conditions of the Foot & Ankle
Many patients with chronic foot and ankle pain have an underlying nerve problem that has not been identified. Peripheral nerve conditions are among the most commonly missed diagnoses in foot and ankle care.
Dr. Bregman's training in peripheral nerve evaluation allows him to identify and treat conditions that other providers may overlook — including Morton's neuroma, tarsal tunnel syndrome, Baxter's nerve entrapment, stump neuromas, and other entrapment neuropathies.
The Diagnostic Challenge
Why Peripheral Nerve Conditions Are Frequently Missed
Peripheral nerve conditions of the foot and ankle are underdiagnosed for several reasons. Standard imaging — X-rays and even MRI — often does not show nerve entrapment or neuroma formation clearly. Symptoms overlap with more common conditions like plantar fasciitis, arthritis, and tendinopathy. And many providers are not trained specifically in peripheral nerve evaluation.
The result is that patients with nerve-related pain are frequently treated for the wrong condition — sometimes for years. They receive cortisone injections, orthotics, and physical therapy that address the wrong problem. Their pain persists. They are told nothing more can be done.
In many of these cases, the underlying problem is a nerve condition that was never properly identified. A thorough nerve-focused evaluation — including careful clinical examination, diagnostic nerve blocks, and appropriate imaging — can identify the true source of pain and open the door to effective treatment.
Signs that your foot pain may have a nerve component
- Burning or electric pain in the foot
- Numbness or tingling in the toes or sole
- Pain that worsens with specific footwear
- Pain that is worse at night or at rest
- Prior treatment has not worked
- Pain that radiates from the ankle into the foot
- Sensitivity to touch in a specific area
- Pain after prior foot or ankle surgery
Conditions Treated
Peripheral Nerve Conditions Evaluated & Treated
Morton's Neuroma
Thickening of the tissue around the nerve between the third and fourth toes. Causes burning, numbness, and sharp pain in the ball of the foot.
Learn moreTarsal Tunnel Syndrome
Compression of the posterior tibial nerve as it passes through the tarsal tunnel on the inner ankle. Causes burning, tingling, and numbness along the bottom of the foot.
Learn moreStump Neuroma
A painful nerve mass that forms at the end of a cut or damaged nerve — often after prior surgery. Causes severe, localized pain that is often misdiagnosed.
Learn moreInterdigital Neuritis
Inflammation of the interdigital nerves without the classic neuroma formation. Often misdiagnosed or undertreated.
Request an evaluationBaxter's Nerve Entrapment
Compression of the first branch of the lateral plantar nerve — a common but frequently missed cause of chronic heel pain that does not respond to standard plantar fasciitis treatment.
Request an evaluationMedial Calcaneal Nerve Entrapment
Entrapment of the medial calcaneal nerve causing pain and numbness on the inner heel. Often confused with plantar fasciitis.
Request an evaluationSuperficial Peroneal Nerve Entrapment
Compression of the superficial peroneal nerve causing pain and numbness on the top of the foot and outer ankle.
Request an evaluationSural Nerve Entrapment
Compression or injury of the sural nerve causing pain and numbness along the outer ankle and heel.
Request an evaluationFeatured Condition
Common Fibular Nerve Injury & Entrapment
Injury or entrapment of the common fibular nerve (also known as the common peroneal nerve) is one of the most frequently overlooked nerve conditions in the lower extremity. It can arise from a variety of causes, including direct trauma, surgeries performed in the region of the knee or hip, and chronic compression. It is also seen in patients with diabetes, where metabolic changes render peripheral nerves more vulnerable to compression and injury.
In some cases, the nerve is injured iatrogenically — meaning as an unintended consequence of a medical procedure. Popliteal nerve blocks administered by anesthesiologists, while generally safe, carry a rare but documented risk of common fibular nerve injury. Similarly, the nerve may be compromised during surgeries involving the knee or surrounding structures.
What makes this condition particularly challenging is that it is frequently misdiagnosed or missed entirely by clinicians who are not specifically trained in peripheral nerve evaluation. Patients are often treated for unrelated conditions — such as lumbar radiculopathy, hip pathology, or generalized neuropathy — when the true source of their symptoms is a compressible or repairable lesion of the common fibular nerve.
When properly identified, surgical decompression or repair of the common fibular nerve is, in most cases, a well-tolerated procedure with a favorable recovery profile. Dr. Bregman has performed over 750 repairs of the common fibular nerve, giving him one of the most extensive documented experiences with this condition in the region. Early and accurate diagnosis is critical to achieving the best possible outcome.
Common Causes
- Direct trauma to the outer knee or fibular head
- Surgeries involving the knee, hip, or surrounding structures
- Prolonged compression (crossing legs, prolonged squatting, casting)
- Diabetes mellitus and peripheral neuropathy
- Popliteal nerve block (rare iatrogenic injury)
- Weight loss with loss of protective soft tissue padding
Symptoms to Watch For
- Foot drop (difficulty lifting the front of the foot)
- Weakness in ankle dorsiflexion or toe extension
- Numbness or tingling over the outer lower leg and top of foot
- Pain along the outer knee and upper fibula
- Gait abnormalities or frequent tripping
Intraoperative Case Study
Common Fibular Nerve Repair: Step-by-Step
The following photographs document an actual surgical case performed by Dr. Bregman — a patient presenting with common fibular nerve injury complicated by dense scar tissue. The procedure progressed from initial exposure through complete neurolysis and protective graft application.* Live surgical images. Viewer discretion is advised.
Step 1
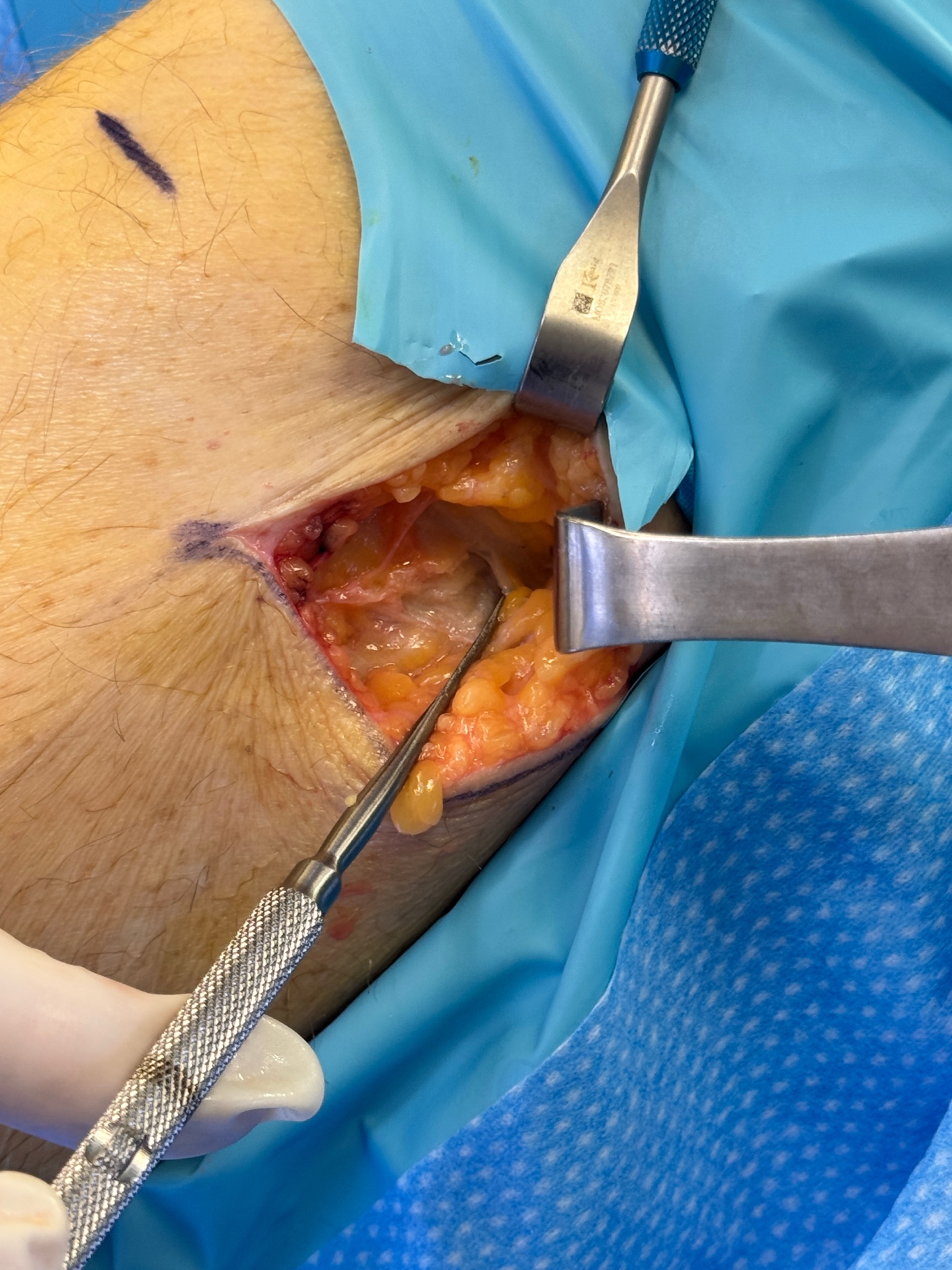
Initial Incision & Exposure
A carefully planned incision is made at the lateral knee to expose the fibular head region. The surgical field is opened to reveal the subcutaneous tissue overlying the nerve.
Step 2

Scar Tissue Encountered
Dense scar tissue is identified encasing the common fibular nerve. This fibrotic tissue is the source of the nerve compression and dysfunction, requiring meticulous dissection.
Step 3
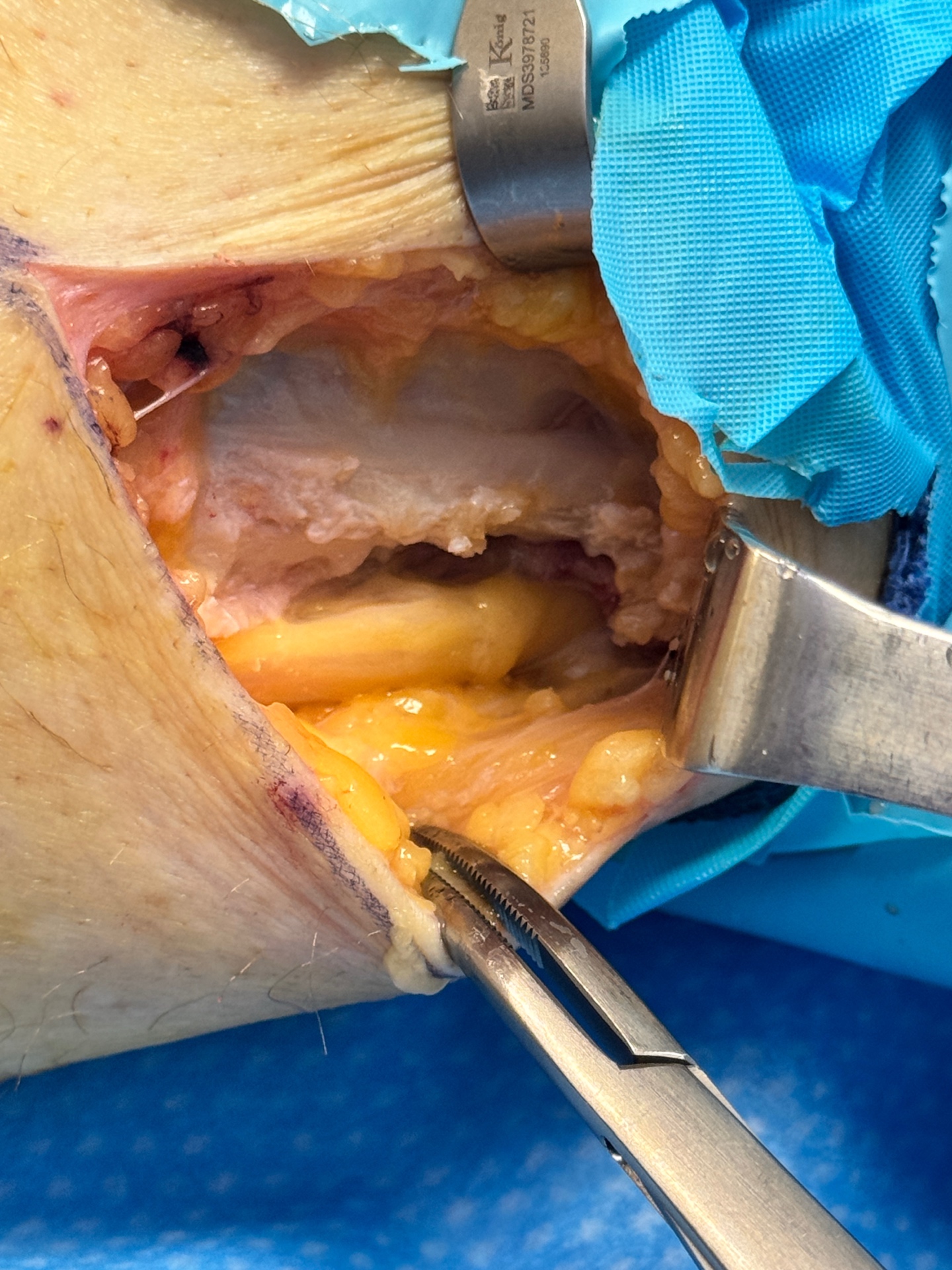
Neurolysis — Nerve Freed
The scar tissue is carefully dissected away from the nerve, tracing it proximally into the popliteal fossa. The nerve is fully mobilized and decompressed along its entire affected course.
Step 4
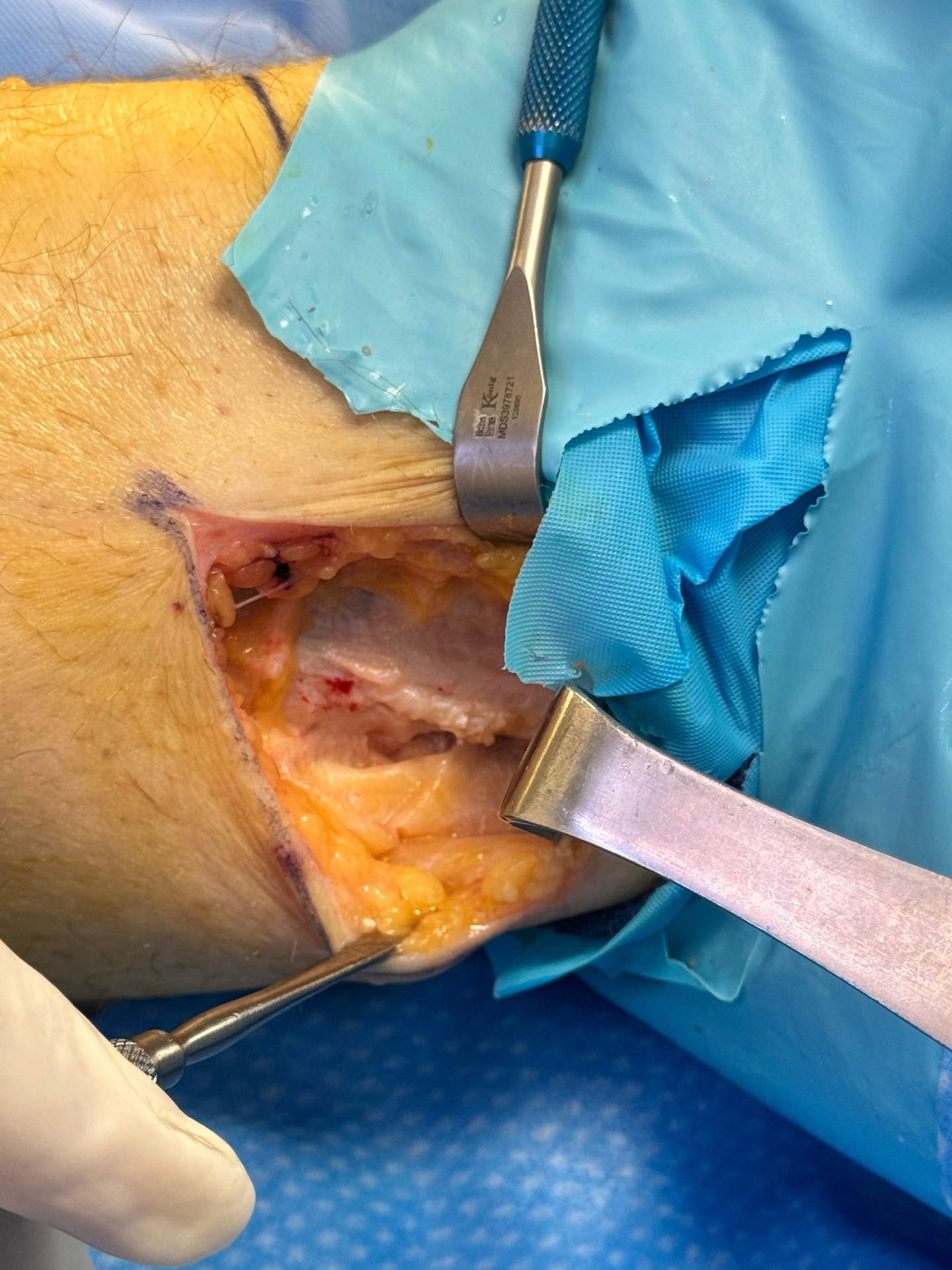
Porcine Graft Applied
A porcine (pig-derived) collagen wrap is applied over the freed nerve to create a biological barrier, preventing re-scarring and protecting the nerve during the healing process.
Patient Testimonial
In His Own Words
The patient featured in the surgical photographs above shares his experience — from the initial misdiagnosis and years of suffering, to his recovery following common fibular nerve repair with Dr. Bregman.
Treatment Approach
How Peripheral Nerve Conditions Are Treated
Thorough Diagnosis First
Treatment begins with a comprehensive evaluation — clinical examination, review of prior imaging and treatment history, diagnostic nerve blocks where appropriate, and advanced imaging if needed.
Conservative & Regenerative Options
Where appropriate, conservative measures are tried first: offloading, orthotics, targeted injections, glucopuncture, and regenerative therapies. The goal is to achieve relief without surgery when possible.
Surgical Intervention When Indicated
When surgery is the right answer, Dr. Bregman performs nerve decompression, neurolysis, neurectomy, and revision surgery for stump neuromas and failed prior procedures.
Schedule a Peripheral Nerve Evaluation
If you have chronic foot pain that has not been explained or resolved, a nerve-focused evaluation may identify the true source of your symptoms.